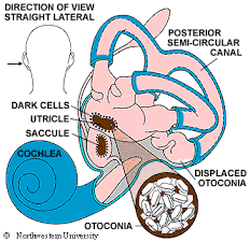
 BPPV This stands for Benign Paroxysmal Positional Vertigo. Benign – not life threatening and not progressive Paroxysmal – sudden attacks, commonly with no initial cause Positional – triggered by head position changes Vertigo – spinning sensation It is the most common vestibular disorder and is curable 80-98% of the time!  What is it? We all have tiny crystals in our inner ear called otoconia. These crystals are so tiny that you can’t even see them on an MRI! Their job is to tell our brain where our head is in space when we move it in different directions. With BPPV, the crystals have come out of place and moved from their usual position inside their sacs into one of the 3 canals above them. Now when we move, instead of sending subtle signals about where our head is, those crystals go flying down the canal and tell our brain that we are spinning with even just small movements. What causes it? For people aged 50 or younger, the most common cause of BPPV is a bump on the head or a whiplash injury. For people over the age of 65, the most common cause is that there is no cause! You just wake up one morning and there it is. What are the symptoms? People with BPPV describe short intermittent episodes of vertigo when moving their head in certain positions. They feel like the room is spinning when they look up or down, lay flat in bed, or roll to their right or left while lying in bed. The spinning is short lived – though it often doesn’t feel like it at the time! It tends to last less than a minute at a time but can come on with each head movement. Sometimes, people with BPPV feel dizzy for a while afterwards and the episodes can cause nausea, vomiting, and a loss of balance. How is it diagnosed? To determine if you have BPPV, we do a test called a Dix Hallpike. It involves turning your head to the side and in a controlled way, dropping you backwards so your head is lower than your body. This test makes most people feel a little yucky, but if you have BPPV, you will get a spinning sensation and your eyes will jiggle a certain way. The way they move tells us where the crystals are hiding in the canals. 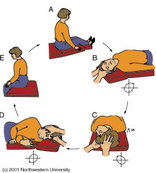 What is the treatment?
Your trained medical practitioner will do a CRM (Crystal Repositioning Maneuver) to move the crystals back into their rightful spot. There are many different maneuvers because there are different spots in the three canals that the crystals can get stuck. Most commonly, the crystals are in the back canal and are free floating in which case an “Epley” maneuver is done. Is it curable? Most of the time, yes. When done correctly, the Epley maneuver puts the crystals back into place 90-98% of the time for posterior canalisthiasis. Often, only one treatment is needed but sometimes repeated maneuvers are required. Occasionally, though rarely, the crystals are very stubborn and won't go back into place. Comments are closed.
|
AuthorPhysiotherapists of Seine River Physiotherapy Archives
May 2020
Categories |
 RSS Feed
RSS Feed
|
We are located on the 2nd floor of the Seine River Professional Center, on St. Anne's Rd just south of Abinojii Mikanah (Bishop Grandin Blvd) and are wheelchair accessible.
Address: 600 St Anne's Rd #220, Winnipeg, MB R2M 2S2 Phone: (204) 415-5006 |
Copyright 2024
Seine River Physiotherapy |